
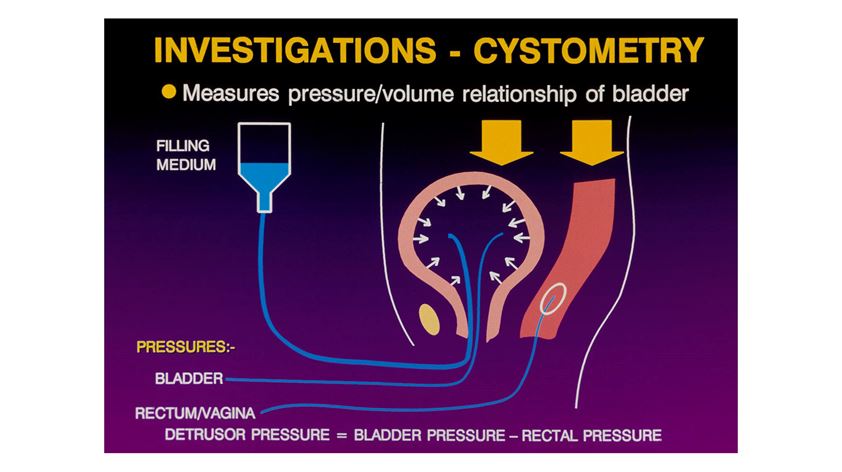
Fig 1: How detrusor pressures are measured during Urodynamic studies

Fig 2: A typical mid urethral sling kit (TVT Exact)
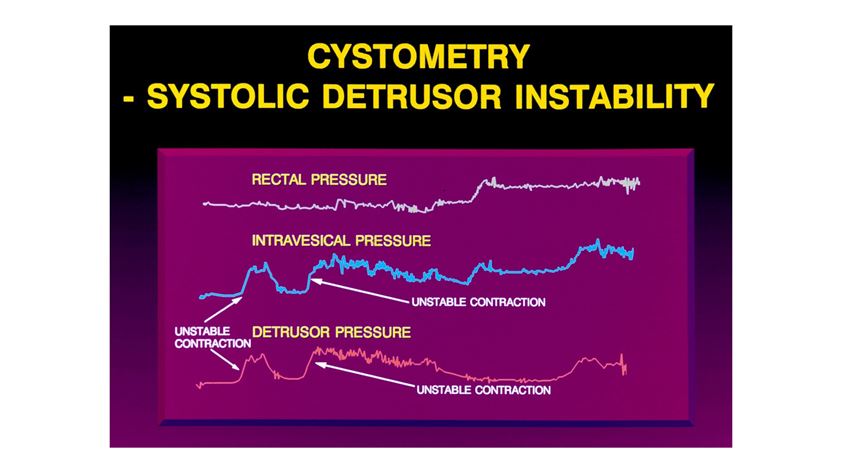
Fig 3: Urodynamic study showing detrusor overactivity

Fig 4: Bladder cancer at cystoscopy presenting with haematuria
A/Prof Christopher Benness
Professor Benness is a certified Subspecialist Urogynaecologist(CU). He is Head of the Urogynaecology Unit at RPA hospital in Sydney. Following graduation from the University of Sydney he trained in both Sydney and London. He has extensive experience in treating prolapse and female urinary incontinence and is active in teaching and research. He is a Clinical Associate Professor at the University of Sydney. Chris is the immediate past Chairman of the RANZCOG CU committee. He consults from the RPAH Medical Centre and his Chatswood rooms and operates at both RPAH and the Mater Hospital.
