
Patient resources Orthopaedics- Knee Replacement

- Home
- Our Hospitals
- St Vincent’s Private Hospital Toowoomba, QLD
- Patient Information
- Orthopaedics- Knee Replacement
Important information for all patients
Please read prior to admission
Welcome to St Vincent's Private Hospital Toowoomba
Thank you for choosing St Vincent's Private Hospital Toowoomba for your joint replacement surgery. This booklet is designed to give you the important information you need to achieve the best outcome from your operation.
It will explain:
- How to prepare for your operation
- What to expect during and after your operation
- How to prepare for your return home from hospital
We recommend you read this booklet thoroughly before your operation. The better prepared you are for surgery, both physically and emotionally, the quicker you will recover from it.
It is, however, only a guide and each person may require differing treatments. It is important that you follow the specific instructions given by your surgeon and treating team.
St Vincent's Private Hospital Toowoomba is a world leader in joint replacement surgery. All our staff are highly skilled in caring for orthopaedic patients, and we use some of the most innovative techniques and technologies in the world.
We assist in your recovery so you can go home from hospital earlier and return to your normal activities sooner. For this to be successful, you need to play an active role in your recovery. Patients who become active participants in their own care achieve better outcomes and will experience:
- shorter hospital stays
- lower infection rates
- shorter recovery with early return to activity
Your registration and admission
We want your hospital admission to run smoothly, so please register your details with us well before your planned admission date. You will have received an Admission Information Booklet from your referring Specialist which outlines all the relevant information you need to know about your Admission.
Out of pocket expenses
We will call you the business day before your admission to explain any excess or co-payments associated with your admission. We ask that you finalise these expenses on admission. If paying a large amount please call 1800 655 099 to arrange an electronic transfer.
If you have private health insurance, please contact your health fund to ensure you are fully covered for your admission.
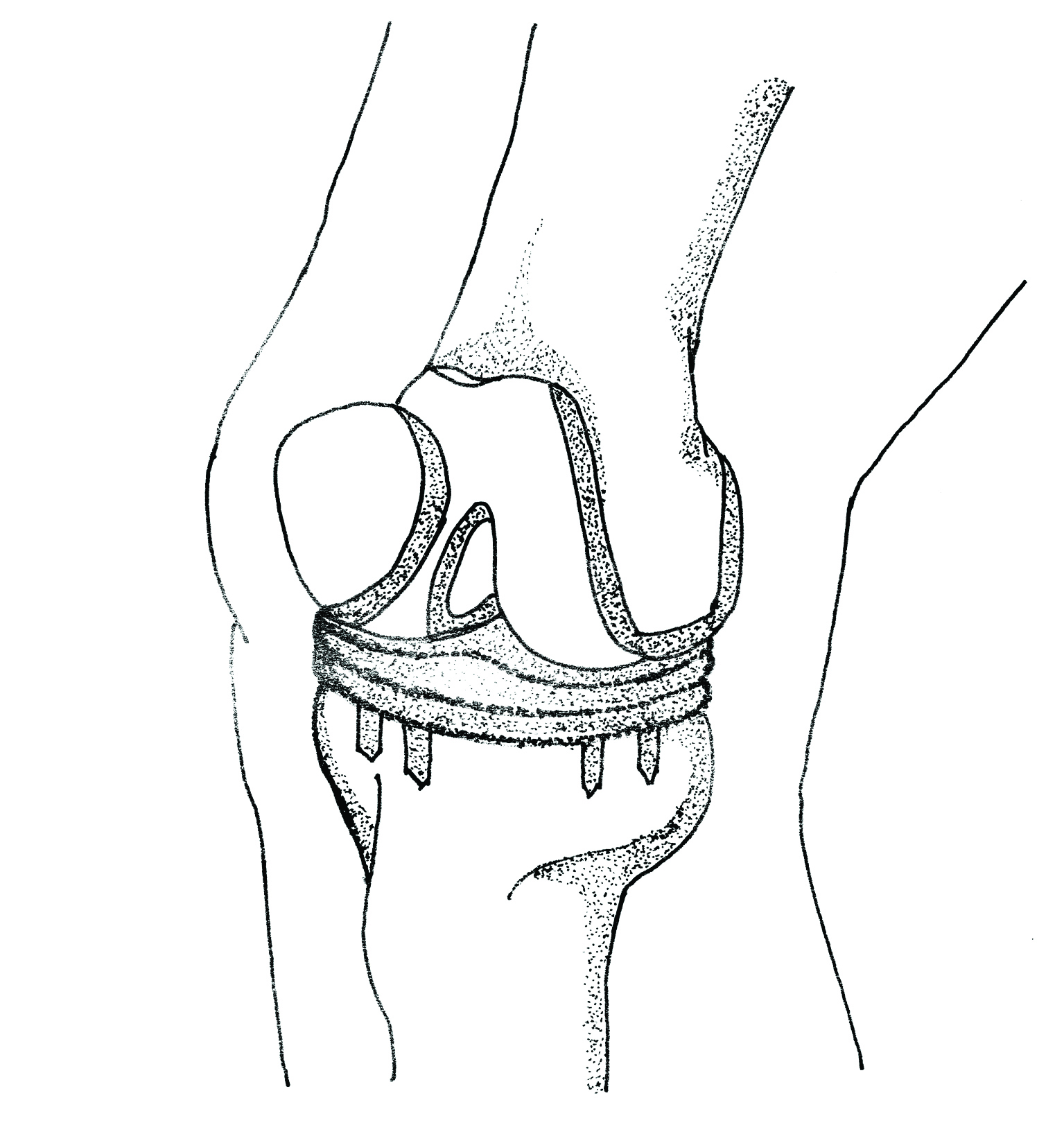
What is a knee replacement?
A Knee Replacement is an operation that replaces a knee joint that has been damaged by arthritis or trauma. Your knee joint is a hinge joint between your thigh bone (femur) and your shin bone (tibia). The knee-cap (patella) moves along the lower surface of the femur. The joint is surrounded by cartilage, muscles and ligaments which enable the joint to move smoothly in its correct alignment.
Articular cartilage coats the joint surfaces allowing free flowing movement of the knee joint.
Arthritis occurs when the cartilage lining the joint is worn away leaving the underlying bone exposed. The joint then becomes rough and distorted, resulting in pain and restricted movement. A limp often develops. As the joint begins to move incorrectly the thigh muscles become weak and wasted. Physical activity often decreases resulting in further muscle wasting.
Arthritis may effect either the medial (inside) or lateral (outside) compartment of the knee. Medial compartment damage is associated with “bowed legs”, called a varus deformity. Lateral compartment damage is associated with “knock knees”, called a valgus deformity. Pain often causes the soft tissues behind the knee to become tight and develop a flexion contracture where the knee is unable to straighten completely.
The Knee Replacement operation replaces the worn lower surface of the femur and the upper surface of the tibia to remove the varus or valgus deformity. The damaged surfaces are removed and then replaced by both a femoral and a tibial component of the prosthesis.
A plastic spacer lies between the two components. If the back of the patella is worn, it may also be re-shaped and re-surfaced with a plastic button. This new joint is designed to ultimately relieve pain, correct deformity, decrease stiffness and improve mobility.
Planning ahead- before your surgery
Your hospital discharge
Discharge planning starts the moment you decide to have your joint replacement surgery. One of the first things you need to do is discuss with your friends or family members who will be able to pick you up and assist with your care when you are discharged from hospital. Most patients are ready to be discharged from the hospital 3-4 days after surgery; however, specific criteria must be met in order to ensure safe discharge (see section – At Home, page 20).
If you have not met the criteria to be discharged home or it has been identified before surgery that you are unlikely to meet these criteria, you may be transferred to our orthopaedic rehabilitation ward. Please discuss this with the staff at St Vincent's Pre-Admission Clinic as soon as possible if you think this may be the case and also talk with your health fund about cover. (see page 19).
St Vincent's Private Hospital supports discharge directly home, where possible, after joint replacement surgery as it has been shown to:
- Promote quicker recovery and return to normal activities
- Reduce infection rate
- Reduce incidence of blood clots
Things to consider prior to your surgery
Prior to your surgery please consider any other health issues or concerns you may have. You may need to book in for a review with your regular consultant prior to your surgery, eg GP, cardiologist, endocrinologist. Ask your surgeon if you are unsure.
Diet and Nutrition
Eat well before you come into hospital. It is important to ensure that your diet is optimal before having surgery. See more on diet in the post-surgery section (see page 10).
Alcohol and Smoking
If possible, please cease smoking four weeks prior to your operation. It is important to note that smoking inhibits the body’s ability to heal, and increases your risk of complications after surgery, such as delayed wound healing and infection.
Smoking is not permitted on the St Vincent's Private Hospital Campus – if you require support whilst in hospital, please let the nursing staff know. You may be prescribed nicotine patches to help in the direct post-surgery period.
You will be asked about your alcohol intake in the admission forms. It is important to note down an accurate reflection of your daily/weekly consumption. Your body may physiologically withdraw from alcohol whilst you are in hospital. This will be monitored if it does occur.
Medications
(See more on this in ‘Preparing for Anaesthetic’, page 10 and "On the day of admission", page 12)
You must bring your medications in original packaging (no pill-boxes, decanted bottles or Webster packs are allowed). This is important for the nursing staff to be able to legally dispense your medication. You will be required to surrender all medications brought into the hospital for the same reason. If you do not bring your own medication in, it will be ordered from the pharmacy. Some diabetic medications which contain Dapagliflozin and/or Empagliflozin may be ceased until you are on a full diet. Please alert your nurse if you are on one of these medications.
Keeping well
In the weeks leading up to your operation, it is important to ensure that you are in good general health. Please notify your doctor’s rooms if you have been unwell in the week prior to your operation. Also, please avoid cuts or abrasions in the week prior to your surgery. If you do have a cut close to the site that will be operated on, your surgery may be cancelled due to the risk of infection.
Prior to your surgery- exercise program and other information
3-4 sessions per day
Studies show that strengthening your muscles before your operation helps you to recover quickly and more successfully. We recommend completing these exercises three to four times a day for 3-4 weeks leading up to your surgery.
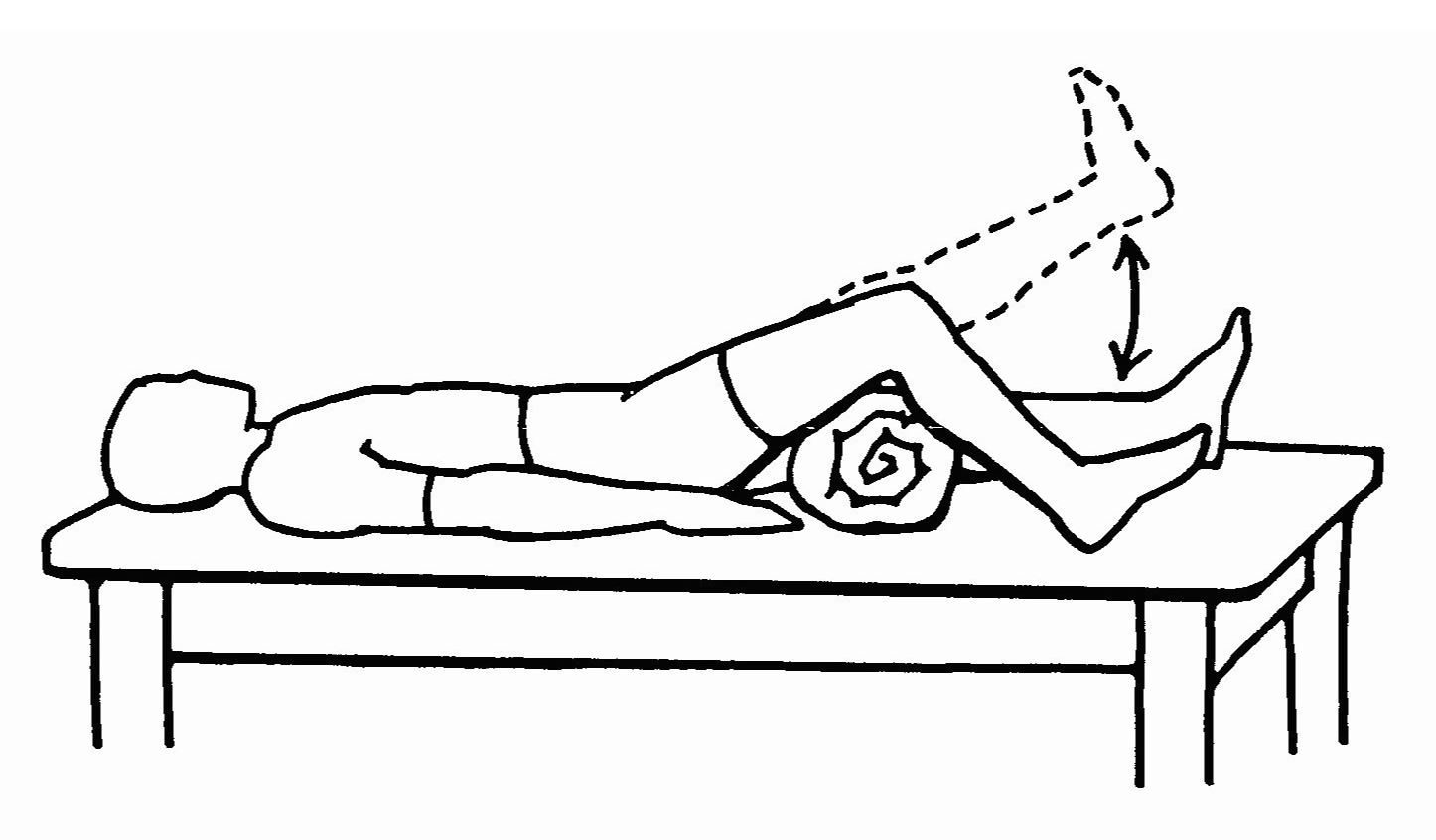
Inner range quadriceps- 10 reps
Place a rolled up towel under the knee. Keeping your thigh down, lift your heel off the bed to straighten your knee Hold for 3 seconds and then lower slowly.
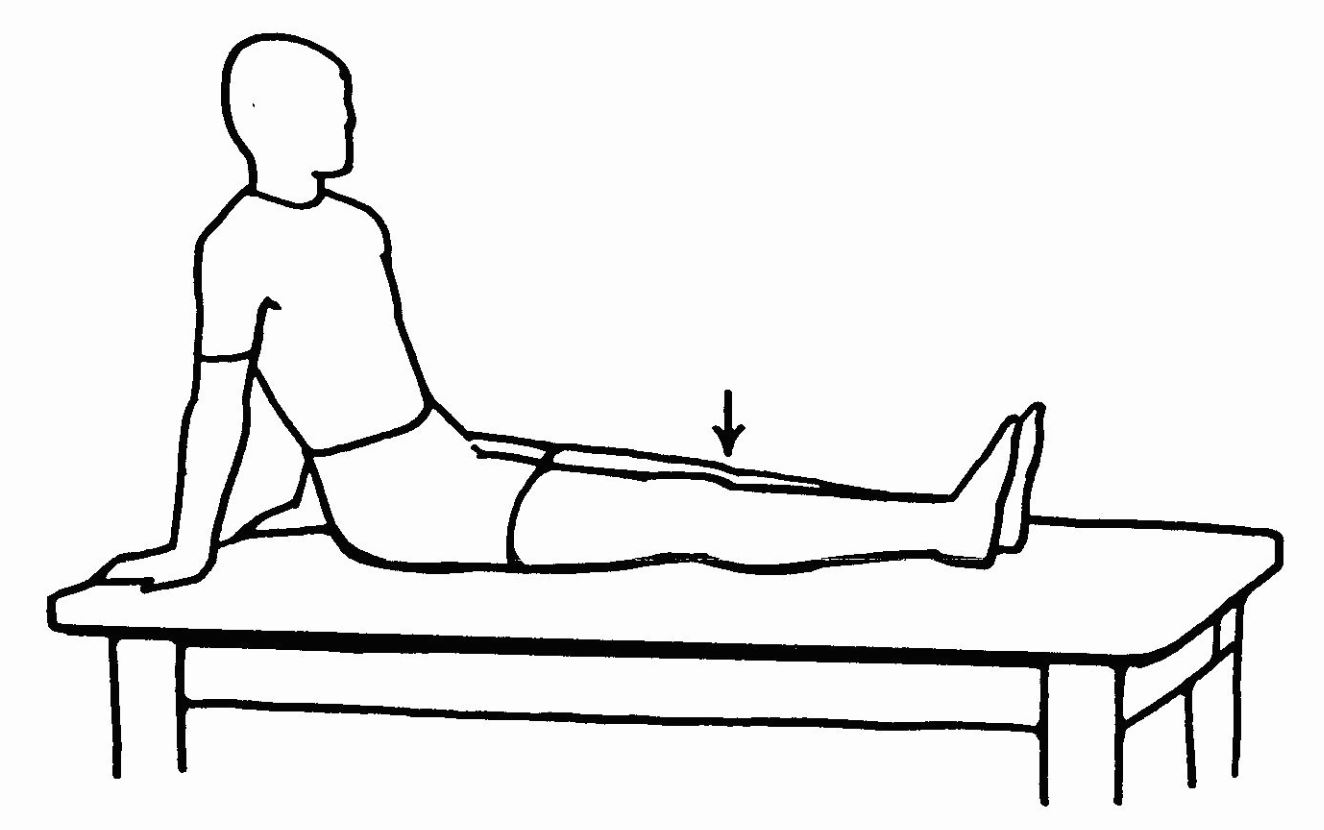
Static quadriceps- 10 reps
Tighten your thigh muscle and push your knee down into the bed. Hold for 5 seconds.
Straight leg raise- 10 reps
Keeping your knee straight, slowly lift your leg off the bed and lower.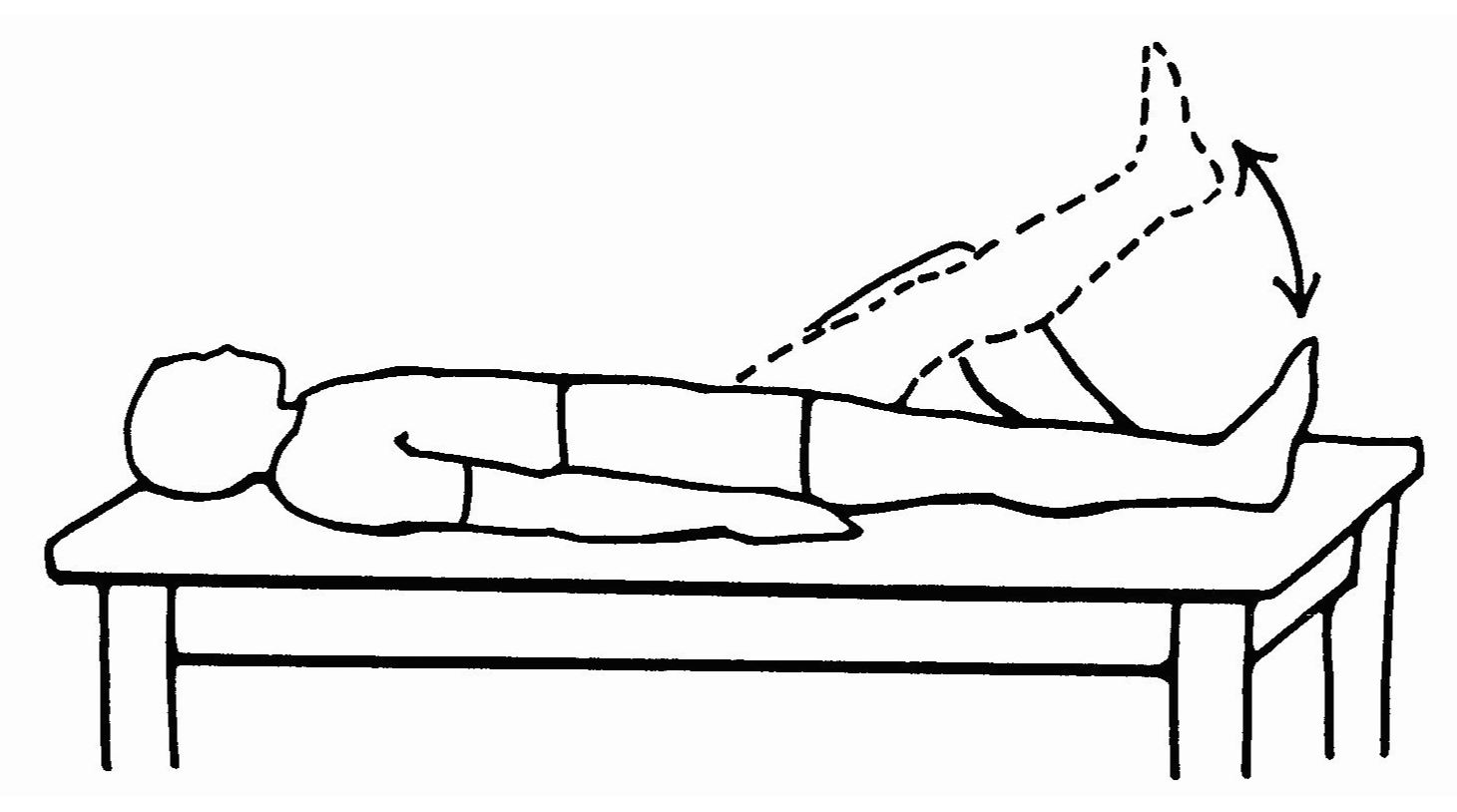
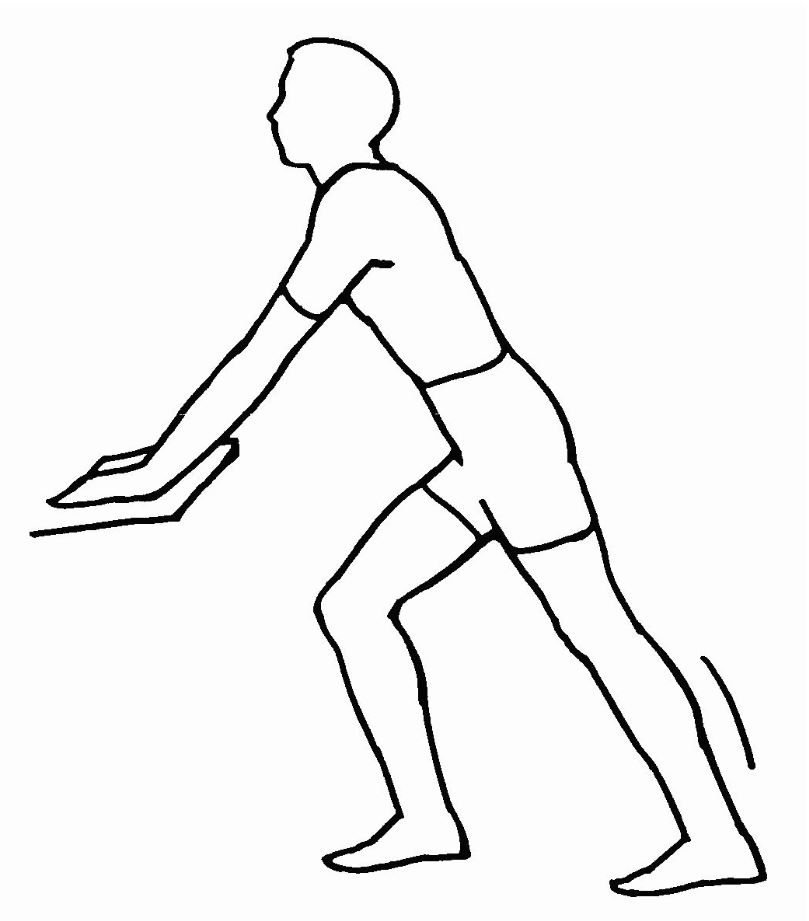
Calf stretch- 3 reps
Place your operated foot back with your knee straight and your heel on the floor. Lunge forward with your unoperated leg until you feel a stretch on your calf. Hold for 20 seconds.
Other exercise
Walking daily, either on land or in a heated pool or cycling are also good low impact options.
Home safety preparation
Setting up your home before your surgery will help to keep you safe, prevent falls, and aid in your recovery. Please read the following suggestions carefully regarding your home set-up.
Trip hazards
Move obstacles such as rugs and extensions cords out of your walk way. Creating a clear, wide path from your bedroom to your bathroom and kitchen will help you to move about easily with crutches.
Make arrangements to keep pets in another area of the house when you first arrive home. Small children may need to be reminded how to interact with you in ways that keep you safe.
Bathroom
Talk to an Occupational Therapist about how to adapt your bathroom to meet your needs during recovery. You may need an over-toilet aid and shower chair which can be hired easily from an equipment store close to your home (See Appendix: Mobility Aids and Personal Care on Page 29).
Seating
After surgery you will need to avoid sitting in low, soft chairs that you may find difficult to get out of. Choose a firm, straight back chair with arms. You may wish to hire an orthopaedic chair or purchase a wedge cushion if you need to raise yourself up higher on your chair (See Appendix: Mobility Aids and Personal Care on Page 29).
Stair climbing
It is okay to climb stairs without assistance if you are able, and you will be shown how to do this by your physiotherapist during your hospital stay with the use of crutches or a walking stick. It may be a good idea to avoid stairs during the night if needing to use the bathroom or leave a light on. Perhaps think about a temporary bedroom set-up to avoid this in the initial few days following discharge home.
Access to items
Keep frequently used items within easy reach to avoid bending or reaching, especially in the kitchen, bedroom and bathroom.
Laundry/cleaning/meals
Arrange for some help with cleaning, laundry and meals in the first few weeks after arriving home from hospital. Freezing pre-made meals and stocking up on non-perishable items will be useful.
Driving
You should not drive until you have had clearance from your surgeon (this is commonly 6 weeks after your surgery). You will need to arrange for someone to drive you to and from any required appointments. For tips on riding as a passenger in the car (see Appendix: Car Transfers on Page 30).
Equipment you will need to organise
When recovering from joint replacement surgery you will require the use of a walking aid for a period of time such as crutches, walking sticks or a frame. Your treating physiotherapist in hospital will advise you on the required aid for discharge home. Crutches are widely available at local pharmacies or mobility stores along with walking frames, should you require one.
These items may be purchased or hired from your local pharmacy or a mobility equipment store. If you would like more information on any of these items we suggest you talk to an Occupational Therapist or Physiotherapist at your Pre-Admission Clinic appointment.
Checklist to complete- prior to surgery
- I have a plan for my discharge home from hospital (eg: do you have someone that will be able to stay with you)?
- I have contacted my health insurance provider and checked I am covered for my hospital procedure and stay.
- I have discussed with my surgeon and family where I would like to attend physiotherapy appointments after I get home.
- I have purchased or hired forearm crutches to use after surgery.
- I have organised equipment I will need at home after surgery such as over-toilet aid, shower chair, high back chair with arms.
- I have appropriate secure footwear to bring to hospital.
- I have comfortable attire to wear in and around the hospital (day clothes and nightwear).
- I have decluttered my home floors to minimise trip hazards.
Preparation for surgery & anaesthetic
Prior to your hospitalisation it is very important that you check with your surgeon, GP or specialist physician about what medications to cease.
- NSAIDs (non-steroidal anti-inflammatory) such as Voltaren, Naprosyn, Celebrex and Mobic may need to be ceased 5-7 days prior to your surgery.
- Aspirin based drugs such as Cardiprin may also need to be ceased 5-7 days prior to surgery. Sometimes these may not be ceased if you have significant heart disease so it is important to check with your surgeon or anaesthetist.
- Anti-coagulants such as Warfarin, Apixaban and Xarelto will also need to be stopped prior to your surgery, after consultation with your doctor. You will need to confirm with your surgeon/ consultant physician or medical practitioner who prescribed the anti-coagulants which date is most appropriate for you to cease taking this medication.
- Generally, Hormone Replacement Therapies and the contraceptive pill need to be ceased 14 days prior to surgery.
- Stop taking herbal products at least two to three weeks prior to surgery, as they can cause unexpected drug interactions, and/or increase surgical bleeding. Fish/Krill Oil tablets should also be ceased.
Please check with your doctor or the nursing staff in the Pre-Admission Clinic if you have any questions in regard to the medications that need to be stopped prior to surgery.
Understanding your anaesthetic
People often think of general anaesthesia as sleep. However, that’s not strictly true. Rather, the anaesthetist puts you into a state of carefully controlled unconsciousness. This is done so that you will not be aware of the surgery. No chance is taken during this period. All your body systems are carefully and constantly monitored by your anaesthetist. Afterwards, we want you to experience as little pain and discomfort as possible. Your anaesthetist will discuss with you your options for pain relief after surgery.
Your role
There are some things you can do which will make your anaesthetic safer.
- Get a little fitter – even a regular walk will work wonders.
- Don’t smoke – ideally, stop at least two weeks before surgery. Call the Quitline 13 78 48.
- No more than one standard alcoholic drink within 24 hours of surgery.
- If you have any kind of health problem tell your anaesthetist and surgeon so they are fully informed.
- If you are anxious and have questions, make an appointment or request to speak to your anaesthetist before admission to hospital and get the answers you need.
- Inform your surgeon/anaesthetist if you object to blood transfusions.
- Inform your surgeon, anaesthetist or consultant physician if you have any problems passing urine which have or have not been investigated or if you have had previous bladder or prostate surgery.
- It is really important to bring your medications to the hospital and a current medication list from your GP or pharmacist.
- If possible, bring any recent reports of relevance such as stress test, angiogram or lung function test.
What should I tell the anaesthetist?
Your anaesthetist will visit you before your operation, to talk with you, and to perform any relevant examinations, if you have not already been seen by an anaesthetist in the Pre-Admission Clinic. Depending on the type of operation, this may not occur until immediately beforehand. The anaesthetist will want to know:
- how healthy you are, if you have had any recent illnesses and also about any previous operations • abnormal reactions to any drugs, or whether you have any allergies
- any history of heart or lung problems or any other medical conditions
- whether you are taking any drugs at present, including cigarettes and alcohol – and, for women, whether they are taking the contraceptive pill. If you are taking prescribed medications, bring them along.
- if you have any loose teeth, wear dentures, caps or plates. Note, if you do have expensive dental work, it may be wise for you to consider getting a mouth guard to protect your teeth.
The anaesthetist wants to have the best possible picture of you and your present conditions so that the most suitable anaesthetic can be planned. Answer all questions honestly – it is really all about minimising risk to you.
Is fasting really necessary? Yes!
The Pre-Admission Nurse will call you the working day before your admission to give you your fasting times. Fasting means no food (including chewing gum) for the specified period before the operation or procedure. However WATER can be consumed up to two hours prior to your surgery, unless otherwise instructed. Water will help maintain hydration and ensure a quicker recovery.
Unfortunately tea and coffee are considered foods. You can have them prior to your surgery, but only according to your food fasting times. If you have taken food within the specified fasting time please tell the nurse on your admission, as your procedure may need to be postponed.
After the operation
Your anaesthetist will continue to monitor your condition carefully after surgery is finished, to ensure your recovery is as smooth and trouble-free as possible.
Once awake, you will feel drowsy. You may have a sore throat, a period of shivering, feel sick or have a headache. These are temporary and will soon pass.
If you have a spinal anaesthetic you may have impaired movement and sensation of your legs for a few hours until the spinal anaesthetic has worn off.
To help the recovery process, you will be given oxygen to breathe, encouraged to take deep breaths and to cough.
Don’t worry if there is some dizziness, blurred vision or short-term memory loss. It usually passes quite quickly.
If you experience any worrying after-effects, you should contact your anaesthetist.
Coming to St Vincent's- what to do on the day of admission
You will receive a phone call the afternoon before your surgery to let you know what time to come in for admission and what time to fast for food and drink. Not fasting from the time instructed may cause a delay or cancellation of your surgery.
DO
- Shower and wash your hair - use an antibacterial soap or wash from the neck down. If you visit the Pre-Admission Clinic the wash will be supplied.
- Remove all nail polish, jewellery and body piercings.
DO NOT
- Eat or drink anything after the time you were instructed.
- Shave or wax before surgery (on admission the staff will use special clippers if you need to be shaved).
- Apply makeup or moisturiser.
Payments
Please bring your credit card or cheque book - any excess, co-payment or amounts not covered by your health fund will need to be paid on admission.
Medications
On the day of surgery:
It is important that you have instructions from your surgeon or anaesthetist regarding your medications prior to surgery, particularly if you are taking one of the following:
- fluid tablets (diuretics)
- immunosuppressant’s or steroids
- blood pressure tablets
- anticoagulants/antithrombotics, eg Warfarin, Aspirin, Clopidogrel, Persantin, Pradaxa, Xarelto
- NSAIDS (non-steroidal anti-inflammatory drugs) eg Voltaren, Naprosyn, Celebrex or Mobic.
- Glaucoma Eye Drops
- Anti Parkinson’s medications
- Anti Depressants
- Reflux medications
- Chronic pain medications
- Diabetic medication
Herbal or natural supplements should be stopped seven days prior to your procedure.
On Arrival
Please visit our Reception Area, Entrance 1 on the lower ground floor for your admission.
Being admitted on the day of your surgery
If you are admitted on the same day as your surgery, you may be directed to the Day Surgery Unit for your admission. Our Pre-Admission staff will inform you where to go for your admission.
If you are admitted through the Day Surgery Unit you will be prepared for surgery by the nursing staff. Your anaesthetist may also undertake an anaesthetic consultation whilst you are waiting. Your luggage will be locked away securely on arrival and will be delivered to your room once you have arrived in your room after surgery. Due to storage restrictions we ask that you keep your luggage size to a minimum. Please be aware that you may arrive before your luggage has been delivered – if this does happen, ask your nurse to ring the Day Surgery Unit to arrange delivery as soon as possible.
Room allocation
Private rooms cannot be guaranteed and are allocated according to availability and clinical/medical needs on the day of admission.
Workers' compensation patients are provided with shared accommodation. A private room can be requested, however the patient will be required to pay the difference and is dependent on the availability and clinical need on the day of admission.
What to bring with you
- The original Registration and Pre-Admission forms, unless you have registered online or previously sent.
- Any relevant doctors’ letters
- You MUST BRING your scans and x-rays on the day of surgery or the operation may be cancelled
- Your Health Insurance Fund Card (if applicable)
- Your Medicare Card
- Health Benefit Card (if applicable) • Pension Health Card (if applicable)
- Bring all medications, tablets, eye drops or injections that you normally take, in their original containers with labels. (Medications cannot be supplied from blister packs). We ask that you give all medications to the admitting nurse so that we can identify the medications and your doctor can review them with you. While you are an in-patient, all medications must be administered to you by a registered nurse and authorised by a Medical Officer.
- Credit Card or Cheque to settle your account
- Comfortable, loose clothes to wear during the day (t-shirts, shorts, tracksuits)
- Night wear (shorts or nighties)
- Toiletries
- Appropriate footwear with secure backing (NO thongs)
- Books and magazines for reading
We ask you not to bring
- Cash (you may only need small amounts for magazines etc)
- Jewellery/valuables of any kind
- Hot water bottle or electric blanket
- Pets
- Plants (eg orchids as gifts)
- Oil burners, incense or candles
- Electrical goods such as hairdryers not electrically tested by a St Vincent's electrician.
(Note: St Vincent's cannot be responsible for any missing items. Each bed side cupboard has a lockable draw for the storage of personal items).
Safety during your stay- committed to high quality, safe care
Preventing falls
The risk of falling while in hospital can be increased after having an anaesthetic or pain relief so it is important to inform us if you have a history of falls. A Falls Risk Assessment is completed for all patients, but knowing about any previous issues will help us to put supports in place to prevent falls. We will discuss these with you and your carer/family when you are admitted.
Preventing pressure injuries
A pressure injury assessment will be completed on admission. Knowing about any previous issues will help us to put supports in place to reduce the risk of pressure injuries.
What you can do to help prevent infection
The prevention and control of infection is everyone’s responsibility including staff, doctors, patients and visitors. St Vincent's is committed to providing high quality care in a safe and clean environment.
Hand hygiene is important
- Wash your hands after going to the bathroom and before eating.
- Don’t be afraid to ask for help if you need assistance.
- Our staff are professional and do not mind being politely questioned or reminded about hand hygiene.
- If you have an intravenous drip, it will have a clear dressing. Do not touch the area if the dressing becomes loose or the area becomes red or painful – tell your nurse and they will check it.
- Do not touch your wound or any other devices such as drip, or drains. Tell your nurse promptly if it becomes loose.
- Keeping the tables and locker uncluttered will assist the cleaning staff to access all surfaces.
What visitors can do to help prevent infection
- Avoid coming to the hospital if they are feeling unwell.
- If visitors have suffered from any form of gastro, they should not visit for 48 hours after symptoms have ceased.
- Children that are unwell or just recovering from an illness should not be brought to the hospital.
- Visitors are welcome to use the hand washing sink or alcohol gel when entering and leaving the wards.
- Visitors should not touch the patient’s wounds or devices.
- Visitors should not sit on the beds or use the patient bathrooms. Public bathrooms are available on each floor.
Returning to the ward after your surgery
The nurse will take your observations each hour for the first four to eight hours, then every two to four hours, to ensure your safety. These assessments will continue overnight and may disturb your sleep. However, this practice is essential to ensure your safety. You will also receive pressure area care whilst your mobility is restricted. This consists of turning you on your side and checking your skin integrity and applying moisturiser. This practice assists in preventing pressure injuries. Your leg will have a bulky dressing and possibly a drain (which will be removed on day one or two) depending on your surgeon’s protocol. You may have TED compression stockings, depending on the protocol of your surgeon. You will also have calf compressors to encourage blood flow and reduce the risk of deep vein thrombosis (DVT).
Getting out of bed for the first time (safe operating procedure)
Moving early and actively participating in physiotherapy is important to the success of your joint replacement surgery and is also critical in helping to prevent complications such as chest infection and DVT (blood clot).
The first time you stand up will be with the physiotherapist and a nurse. Depending on your surgeon’s protocol and the time you arrive back from theatre, this may be on the same day as your surgery. The nurse will take your blood pressure in a lying position. The physiotherapist will then guide you to sit on the edge of the bed. Your blood pressure will be taken again after two minutes. You will stand using a walking frame with the physiotherapist if you are feeling well enough. Do Not attempt to get out of bed alone.
Clinical handover
As part of our clinical practice the nurse handover, at the end of each shift, will take place in your room – this means that you will be kept up to date with your care plan, given the opportunity to be involved in decisions about your care and ask questions about any aspect of your stay or treatment. Clinical handover by the nursing staff takes place at the following times:
6.30am – 7.00am Night shift to Morning shift
14.30pm – 15.00pm Morning shift to Afternoon shift
22.00pm – 22.30pm Afternoon shift to Night shift
Room service/meal service
All meals are freshly prepared and made to order at your convenience and delivered to your room. These can be ordered between 06.30am and 18.30pm. Visitor’s meals can be ordered through our Room Service at a cost to you. If you are on a diet that has special requirements, including allergies, intolerances and preparation for a procedure or after surgery, menu choices may be modified or restricted. We can also cater for cultural needs such as Halal and Kosher, please speak to your nurse or room service assistant. A menu with information about room service and how to order will be on your bedside table.
Deep breathing and circulation exercises
You should commence the following exercises as soon as you wake up from your operation:
Deep breathing and coughing – repeat every hour
- Take 5-10 deep breaths every hour, holding the breath at the top for a couple of seconds, followed by a strong cough.
This will help your lungs to remain fully expanded after the effects of your anaesthetic and help reduce the likelihood of a chest infection.
Circulation exercises – repeat every hour
- Move both ankles and feet up and down for 20 seconds
This will help to minimize the risk of a blood clot (DVT).
Pain and swelling management
St Vincent's Private Hospital employs advanced pain management techniques to optimise your comfort after joint replacement surgery.
Pain will vary from person to person. Patients are typically surprised at how manageable the pain/ discomfort in the operated region is, even early on after your joint replacement. This is achieved through the advanced skills of our specialised surgeons, in combination with the pain management expertise of our anaesthetists, orthopaedic nurses and physiotherapists.
By using a combination of medications/techniques (multi-modal pain management) the degree of pain experienced is substantially reduced following your surgery. This allows you to move about earlier following your joint replacement and confidently return to being independent within a relatively short period of time. Due to optimised pain management, many patients find they can reduce their medications within several days post-surgery and not experience any increase in pain.
Swelling in your hip and leg is a normal part of the healing process and you should not be worried.
Our staff will give you ice packs to help reduce swelling and show you how to elevate your leg in bed.
Note: Heat packs should not be used.
Nutrition
A well balanced diet after surgery will assist your body in the healing process. Caloric (energy) requirements increase whilst you are in hospital – it is important not to lose weight directly after your operation due to the increased caloric requirements – remember your body is trying to heal a wound. Maintain a high fibre and high nutrient diet after the operation in order to help with constipation and healing respectively. Try to avoid highly processed foods, and opt for lean protein, whole fruits and vegetables and whole grains after the surgery.
If you are diabetic, it is especially important to monitor your glucose levels after surgery and be mindful of your intake. Your blood sugar levels may vary from your norm after surgery and in some cases patients may require insulin or increased doses of insulin whilst in hospital. If you require advice from a dietitian, please let the nursing staff know.
Output urine/bowels
Your urine output will be monitored hourly if you have a catheter. The nurse will assist you with your toileting needs. The catheter may be removed on day one or two if you have one. Passing urine after a catheter can vary – this will be monitored by the nursing staff to ensure that passing urine has returned to normal. You will also be given laxatives for your bowels. The combination of the anaesthetic, pain relief and reduced mobility can lead to constipation if early intervention does not occur. You should have your bowels opened before leaving the hospital. Severe constipation can cause nausea and other complications. This may occur if your bowels have not been open for several days, and further treatment may need to be initiated. Please let your nurse know if you are starting to feel unwell or uncomfortable.
Teaching and emotional support
Throughout your stay at St Vincent's there will be a range of services available to assist you with both the physical and emotional challenges of joint replacement surgery. This will include medical staff, nursing, allied health, and pastoral care. Please don’t hesitate to voice any questions or concerns you may have during your stay.
Your recovery- days 1-3 after your operation
Physiotherapy after joint replacement surgery is an essential part of your recovery to help you restore muscle strength, joint range of movement, walk normally again and complete personal care tasks.
Mobility/physiotherapy
Even if you have already been up on the day of your surgery, the first time you get up on the day after your surgery will also follow our Safe Operating Procedure. This means a nurse and physiotherapist will be there to help you stand by the bed with a frame and possibly walk a short distance. Do not attempt to get out of bed on your own. Your physiotherapist will let you know when it is safe for you to get up by yourself.
You will see a physiotherapist on the ward after your joint replacement surgery. It is a normal part of rehabilitation to feel pain during and after your therapy sessions and it is important that you take your pain relief prior to your sessions so that you can actively participate as best you can.
Your physiotherapist will also teach you hip exercises to do in your bed. These exercises are for you to do independently throughout the day. This is essential in order for your joint replacement surgery to be successful. It may also be appropriate for you to start sitting in a chair for some of your meals — your physiotherapist and nurse will advise you when it is safe to do so.
Throughout days one to three after your operation you will continue working towards your goal of going home by (day 3 after surgery) or as per your surgeon's requirement.
A physiotherapist will see you daily to:
- progress your exercise program
- practice your walking with crutches or sticks
- practice stairs
- sit out of bed.
An occupational therapist may assess you to see what equipment you may need at home. They will guide you on the best place to hire any equipment such as shower chairs and over-toilet aids if we feel that you need them to go home.
(Refer: Appendix: Mobility aids and personal care on page 29)
Tests and procedures
You will have blood tests performed during your admission, depending on surgeon preference. A post-operative x-ray of your hip will take place post-op or day 1. Sometimes a CT scan is also required, depending on your surgeon. You may also have swabs of your nose, groin and wound taken to screen for infection.
Discharge planning
If patients have support at home from friends or family, studies show they recover quicker at home. Therefore St Vincent's supports discharge directly home following your operation, and will start discussing this with you straight away.
If it looks as though you might not meet the criteria to safely go home, your nurse, physiotherapist or surgeon will discuss other options with you. We will ensure that you have been referred to outpatient physiotherapy/private physiotherapy for when you do get home.
Going home- days 3-4 after your operation
Criteria for discharge
It is important that you actively participate in your therapy sessions so that you can meet the following criteria as soon as possible in order to discharge home. Timely discharge is important to help improve your function, reduce the risk of infection and reduce the risk of DVT. The criteria for your discharge are:
- your medical condition is stable
- you are emptying your bladder and have had your bowels open
- your pain is controlled with oral pain medication
- your home is prepared for your safety
- correctly getting in and out of bed either independently or with minimal assistance from your family/friend who will be staying with you on discharge
- walk independently around the ward using assistive devices (crutches/walking stick)
- climb stairs, if necessary
- safely perform personal activities of daily living such as getting on/off toilet and showering with minimal assistance.
Discharge time is 10.00am, please arrange for someone to pick you up at this time.
On discharge, a discharge summary letter will be provided with instructions specific to you. You will also get a copy to give to your local GP as it is recommended you keep in touch with her/him. Any x-rays you have had during your stay are your property so make sure you check that you have them to take home.
Your regular medications will be returned to you. Typically you will go home on some pain medication. The pain/discomfort will progressively resolve with time. You should not experience severe pain once at home, nor for prolonged periods during your rehabilitation/physiotherapy. Should this occur you should consult your GP who will prescribe appropriate medication for your pain. A pharmacist from St Vincent's will discuss any new medications with you prior to discharge. Remember you may also be required by your surgeon to take blood thinning medications for some time once discharged.
Your surgeon may see you prior to discharge and tell you when to arrange a follow-up appointment if you have not already made one. The time of your follow-up appointment after surgery will depend on your surgeon.
You will need to speak with your ward nurse about having your wound checked once you go home.
At home- your recovery
The staff at St Vincent's will help you to prepare as best you can for your discharge home. It is normal to feel worried about going home, and remember you will need to have a support person such as a friend or family member that can help you out in the first few days at home. You can expect a gradual improvement over the coming months, with a gradual lessening of pain, stiffness and swelling. You will gradually begin to return to a more independent lifestyle.
Pain management
Remember you need to take your pain medication as soon as you feel discomfort. Do not wait until you have severe pain. Follow the instructions given by the nurse or pharmacist on discharge. If you are unsure of your pain medication schedule please contact your GP. After exercise you should ice and elevate your leg for 20 minutes. This will help reduce swelling and pain.
Sexual activity
During sexual activity, it is best that you use positions that avoid bending your hips too deeply or for extended periods. Let your partner take the active role. Please be mindful of your hip precautions during this activity.
Diet and constipation
Proper nutrition is needed for healing. You may not be very hungry but it is important you try to eat and drink small amounts as this will aid in your recovery and give you energy to participate in your exercise program. Pain medication can cause constipation, this is a very common problem. Things that will help constipation include a high fibre diet, plenty of water, and walking as much as comfortable. If you continue to have issues with constipation please seek advice from your local pharmacist, or GP.
Wound care
For the first 10-14 days your wound is still healing. You might experience slight itching which is normal. If at any point there is ooze, the wound is hot and very red, and you feel unwell let your surgeon or GP know as soon as possible. Your nurse will discuss with you how to care for your wound at home. Wound care will be specified on your discharge paperwork. You will be instructed by your nurse prior to discharge when to see your doctor or GP for a wound check and possible removal of sutures (some surgeons now use dissolving sutures). You may be supplied with spare dressings when leaving hospital. If you do need to change the dressing for some reason, follow instructions per the instructions given on discharge.
When to notify your doctor
If you notice any of the following, you should contact your surgeon immediately:
- increasing pain at the operative site
- new redness or warmth
- new or increased ooze from your wound site
- the operated joint is becoming increasingly swollen
- your calf becomes swollen, red or tender
- a high temperature and you feel unwell for more than 24 hours
- if your knee is becoming very hard to flex (bend) or is not improving since you were discharged.
- you experience shortness of breath or chest pain please see your nearest doctor or emergency department.
Continuing Physiotherapy- Physical activities at home
Continue your physiotherapy exercise program and gradually increase your walking distance and frequency as you feel comfortable. You should use the walking aid prescribed by your physiotherapist to decrease the risk of falling.
Ensure you attend any scheduled physiotherapy appointments.
Below are some of the activities you should be aiming to accomplish during the first 6 weeks. Keep in mind everyone is different and will improve at a different pace.
- walk without help on a level surface with your walking aid (frame, crutches, stick) for as long as you feel comfortable, start with 5-10 mins
- ascend / descend stairs
- get in and out of bed independently
- get in and out of a chair independently
- shower independently, either sitting or standing •resume activities of daily living including meal preparation, light chores, walking and going outside the home for social activities.
- you may be able to return to work, depending on your occupation. This is very individual and you should talk to your surgeon and physiotherapist.
Walking
Walk as normally as possible, try to avoid limping. This means you will likely need to use crutches or a walking stick until you can take full weight through your leg without a limp. Your operated leg should try to match the action of your other leg. As your muscle control and hip flexibility improve, your confidence should increase allowing you to progress your walking distance so that you are managing 30 minutes by about the six week mark.
(See Appendix: Mobility aids and personal care on page 29).
It is important to be able to walk correctly, not just to be able to walk.
The main aspects of walking that people need to work on after a knee replacement are;
- Straighten your knee and land on your heel when your foot reaches the floor
- Push off with your toes when your foot is behind you
- Bend your knee as you swing your leg through
Sitting
Do not sit for longer than 45 – 60 minutes at a time as your knee will become very stiff. When you sit, you should sit in a firm chair with arm rests. Step back so that you can feel the chair behind your knees, let go of your walking aid and hold onto the arm rests of the chair. Lower your bottom down and slide the foot of your operated leg forward. This prevents a sudden bend of your knee. You should then bend your knee so that your feet are under the chair.

Showering
It is recommended that you use a shower chair until you have adequate strength in your hip and good balance. A shower can be more tiring than you think, so ensure you have the strength and energy to be able to endure standing up in the shower before you try.

Tips for a better recovery at home
- Do not sit for longer than 45 – 60 minutes at a time. You may nap if you are tired but do NOT stay in bed all day.
- Frequent, short walks are best and key to a successful recovery.
- Take your pain medication 30 minutes prior to exercises or heading out for a walk.
- Elevate and ice your knee after doing your exercises/walking for 20 minutes to help reduce swelling.
- You should ascend/descend stairs with support – hold onto the railing and climb up as instructed by your physiotherapist (see opposite).
- You may experience difficulty sleeping at night. This is a normal part of the recovery process. Ensure adequate pain medication prior to sleep and try a cold pack on the joint before bed. Getting up and moving around may also help relieve the discomfort.
- Do not resume driving until you have discussed this with your surgeon. You may be a passenger in a car.
- Plan your day so you only spend small amounts of time doing different tasks. Remember that you need to rest when you are tired.
- Consider shopping for groceries on the internet or shop with someone who is happy to carry items for you.
Recovering at home- do's and don'ts
Stairs
Your ward physiotherapist will teach you how to go up and down stairs safely and confidently. It is a good idea to practice with your crutches before your surgery. The technique is:
Up Stairs
- Unoperated leg (Good leg)
- Operated leg
- Crutches/Stick
Down Stairs
- Crutches/Stick
- Operated leg
- Unoperated leg (Good leg)
Both legs and the crutches should all move to the same step.
IMPORTANT: If the exercises are ceased, your hip will not stay at the current functional level – it will decrease. We recommend you gradually increase walking, concentrating on reducing your limp.
Your independent exercise program should be continued for six months to allow your new knee to achieve its maximum potential. If your range of movement is lost or decreases or you have any concerns please contact your surgeon.
What to do
- Walk and do your physiotherapy exercises daily
- Make follow-up appointment with your surgeon
- Continue to take tablets for pain relief as required
- After exercise elevate leg and apply ice to knee for 20 minutes.
- Limit time sitting to maximum 45 minutes
Please adhere to the following:
- Avoid sitting in low chairs
- Avoid deep squatting, jumping, running, high impact sports, or attempt kneeling until advised
- No driving for six weeks – discuss this with your surgeon.
What to expect
- Some swelling and bruising to area
- Some associated pain after attending exercises
How do you know everything is OK?
- You are coping with your pain and you are comfortable
- Your wound is healing
- You are able to dress yourself
- You are wearing your anti-embolic stockings/ anticoagulants (as instructed)
- Your appetite is returning
- You are safely moving around your home
Further precautions
- Dental procedures - check with your Doctor regarding prophylactic antibiotics and when to cease anticoagulants (blood thinners)
- Air travel – if travelling within six weeks of surgery contact your doctor to discuss any precautions.
Frequently Asked Questions
When can I walk without a stick?
The most important aspect of walking is that you walk without a limp, which you may have developed while protecting your knee prior to your operation. Therefore, you are allowed to stop using the walking stick when you are able to walk without a limp. Your Physiotherapist will advise you when you are ready to begin walking without a stick. Remember, people are more careful when they see someone with a walking stick, so you may be better off using your stick when you will be in crowds, or on uneven ground until you are very confident.
When will the pain go away?
Everyone’s pain varies after a hip replacement and it takes time for the pain to gradually settle down and go away. It is not uncommon to have some pain or discomfort in your knee for up to six to nine months after surgery.
When can I return to driving?
You may begin driving at six weeks after your operation. If you have had a left knee replacement and have an automatic car, check with your surgeon as to whether you can begin driving sooner.
Can I kneel on my knee?
Some Orthopaedic Surgeons allow you to kneel directly onto your knee after about six weeks if you feel comfortable doing so. Check with your surgeon first at your follow-up appointment.
Can I rest with a towel or cushion under my knee while on the bed?
No, this stops the blood from circulating in your lower leg, increasing the likelihood of getting a clot in your leg. It also prevents you from fully straightening your knee.
Can I go to the dentist?
You can go to the dentist but you MUST contact your surgeon regarding prophylactic antibiotics if you are having any dental procedures done to reduce the risk of an infection travelling to your knee.
When will the swelling go away?
It normally takes three to four months for the swelling to settle down. Continue to put ice on your knee and have your knee elevated for 20 minute periods throughout the day by lying down, especially after exercising and long walks. Although the swelling does limit your knee bending, it is detrimental to your knee to wait until the swelling has gone away before you start pushing your knee to bend, as the scar tissue in your knee will have developed by that time, causing a permanent restriction in knee bending.
When can I begin gym work/weights?
You may begin cycling on a stationary bike two weeks after your operation. After six weeks you may begin using weights on your legs. You should begin with low weights and gradually increase them. Check with your physiotherapist prior to beginning weights or gym work. It is not advisable to do any regular jogging, running or jumping activities after your surgery as it will cause your knee replacement to wear more quickly.
When can I return to bowls, golf or tennis?
You can return to bowls and golf three months following your knee replacement surgery. You are permitted to return to social doubles tennis at this stage also, but you are advised not to return to competitive tennis as it will cause your knee replacement to wear out more quickly.
Sexual activity?
During sexual activity, it is best that you use positions that avoid bending your knees too hard or for extended periods. Let your partner take the active role.
When can I travel on a plane?
You can travel on an aeroplane when you are comfortable and when your surgeon is happy for you to do so. It is likely your surgeon will ask you to take specific blood thinning medication to reduce the risk of you developing a DVT. Please ask your surgeon if you are planning any travel.
General Information
To make your stay as pleasant and comfortable as possible we provide a wide range of patient services.
Pastoral care
Pastoral Care staff are employees of the hospital that work as part of the interdisciplinary team to provide emotional and spiritual support to all patients regardless of faith, beliefs and religion. They aim to visit every patient at least once to offer emotional and/or spiritual support. Visiting Chaplains are available to minister to other faith denominations as requested.
Chapel
The Chapel is located near the main entrance. It is open at all times for prayer to people of all faiths, or as a place of solitude and reflection.
Healing garden
A serene haven for quiet reflection and comfort, the garden is available to patients, visitors and staff. The garden is located in the central courtyard on the ground floor.
Volunteers
Our volunteers make a highly valued contribution to St Vincent's. They assist our staff in greeting patients and visitors, escorting patients to their rooms and with tasks like caring for flowers.
Coffee shop
Pulse Café is located on the Lower Ground floor of the hospital at Entrance 6 (Emergency Department).
Pharmacy
The Pharmacy is located on the lower ground floor and provides a full range of medicines.
Smoking
Smoking is not permitted in any building, vehicle or area within 5 metres of the St Vincent's Hospital Campus.
Confidentiality & privacy of information
St Vincent's Private Hospital will safeguard the privacy of personal information obtained from you whilst you are in our care. We respect and will uphold your rights to privacy protection under the National Privacy Principles contained in the Privacy Act 1988. '
For more detailed information on Confidentiality and Privacy of Information see our brochure “Privacy and Your Health Information”, or the “Patient Information Privacy” page on our website.
Appendix 1- Blood Transfusion/Blood Product
Indications for having a blood transfusion/blood product:
Like all medical treatments, a blood transfusion should only be used when really necessary. The decision to give a blood transfusion to a patient is made only after careful consideration. A transfusion may be necessary to replace part of your blood, and is given either:
- to replace red blood cells to treat or prevent anaemia, improve oxygen transport and relieve symptoms of dizziness, tiredness or shortness of breath
- to give platelets to help stop bleeding by helping your blood to clot
- to give plasma or plasma derived products to stop and treat bleeding by helping your blood to clot.
Alternatives to blood transfusion:
- preoperative assessment and treatment to ensure that blood levels are maximized before any planned surgery eg Iron infusions
- fluid replacement
- use of Artificial compounds and/or iron supplements
Discussion with your doctor may be necessary, as some methods of treatment may not be suitable for your case.
Risks associated with a blood transfusion/blood product:
- common mild reactions: fever, hives, skin rashes, temperatures, general unwell feeling
- severe rare reactions: kidney failure, shock, transmission of an infectious agent.
- allergic/immune complications between the patient’s blood cells or immune system and the donated blood.
Consent
Consent must be obtained if a blood transfusion is necessary. This is a requirement of the QLD Health Department. Consenting means you understand why you need a transfusion, as well as the risks involved and benefits for you. Please look at the link provided below for further information.
The Australian Red Cross Blood Service – Information for Patients
Appendix 2- Bone Graft Information
Bone graft information
Some surgical procedures require the use of bone or tissue grafts (allograft). In some instances your surgeon may be able to use your own bone and tissue (autograft) for your surgery; however for complex procedures a donated graft may be required. The use of allograft (tissue donated by another person) is necessary due to the limited availability of your own. This reduces the time under anaesthetic, pain from a potential second surgical site, loss of mobility, and risk of infection at the second surgical site.
Where does the graft material come from?
There are two donor programs:
- Patients having hip replacement surgery can donate the ball part of the hip joint (femoral head Australian Tissue Donation Network).
- During their lifetime people may indicate a wish to donate organs and tissue after their death. Like organ donation, with the consent of the next of kin, the retrieval of bone and associated tissue such as tendons, ligaments and fascia can occur by the Australian Tissue Bank.
All Australian Tissue Banks are regulated and licensed by the Therapeutic Goods Administration, which is the auditing body of the Commonwealth Department of Health and Ageing.
How are donors screened?
There are strict donor selection criteria and regulatory controls related to the screening and testing of donors and donated material. A thorough review of the donor’s medical and social history is obtained prior to donation and again before graft is released for transplantation. A variety of laboratory specimens are collected from the donor for routine testing, to exclude infectious and/or transmissible diseases. The donor’s blood is tested in the laboratory for a wide range of diseases including:
- Syphilis
- Hepatitis B & C
- HIV (AIDS)
Swabs are cultured to ensure there has been no contamination during the collection or processing of the tissue. The graft is irradiated as the last processing step.
What is the risk of transmission of disease?
Bone and tissue transplant procedures are very common. The demand for human graft materials is growing, and bone and tissue donations assist many patients undergoing complex surgical procedures, thereby improving mobility and function. There is a remarkable record of safety with tissue grafts and strict regulatory controls monitor the donation and transplantation of tissue in Australia. You should be aware that even with rigorous testing procedures, there does remain a very small risk of disease transmission. However, it is very important to reiterate, it is an extremely low risk and there are exhaustive steps taken to ensure screening, testing and processing are performed according to strict regulations and guidelines.
How can the donated bone & tissue be used?
Donated bone and tissue is very valuable for use for surgical treatment of patients who may require a transplant, eg:
- bone tumour surgery
- spinal surgery
- hip revision surgery
- a variety of general orthopaedic procedures
- dental bone loss and maxillofacial deformity and reconstructive surgery.
It is not necessary for the donor and recipient to be tissue matched, as for the transplant of organs. However, the Rhesus factor is matched where possible for female recipients of child bearing age. Bone grafts are often used in conjunction with prosthetic implants such as metal hip implants, plates and screws. Once implanted into the recipient the bone graft does not grow, but stimulates the recipient’s bone to grow into the graft to repair areas of lost bone.
Consent to receive graft material
Your surgeon, or a doctor in the hospital, will discuss with you the use of graft for your operation. You will be required to read and sign a specific consent to receive a graft. If you are uncomfortable with any detail in the consent form or have any questions, you should discuss this with your surgeon.
What happens to the graft after the transplant?
Bone and tissue grafts don’t grow. They are incorporated into the recipient’s body through conversion into new bone or soft tissue.
Will I have to take ‘immunosuppressant’ drugs after surgery?
Unlike patients who receive organ transplants (such as kidney or heart transplants) it will not be necessary for you to take any medications specifically related to tissue rejection. You may however be prescribed other medications such as antibiotics, following your surgery.
Is there any cost associated with receiving a graft?
There is no payment made to the donor or donor family for the donated material, nor is there a cost to them. Australian law prohibits the sale of human tissue. However, a ‘fee for service’ is approved by the Commonwealth for each graft transplanted. These graft fees are charged to the hospital, and are fully recoverable through the private health funds, or through Medicare if the surgery is performed in a public hospital.
Fees for the supply of graft items incorporate the many costs associated with providing the material, such as laboratory costs, consumables used in the retrieval and processing of the graft, regulatory and quality system costs and administration costs such as staff wages and insurance.
For Further information:
Perth Bone and Tissue Bank Inc.: https://www.pluslife.org.au/about/our-recipients
Appendix 3- Rehabilitation - your options
The Rehabilitation Unit offers a specialised, multidisciplinary rehabilitation program tailored to the individual’s needs and goals. Our staff helps patients regain their physical function and daily living skills with the aim of returning them to their previous lifestyle.
On admission
A full clinical assessment will be undertaken at the time of your admission. This assessment includes:
- your temperature
- blood pressure
- pulse
- ECG
- urine testing
- post residual bladder scan
- blood sugar
- chest x-ray (if required)
- weight and blood tests.
Any abnormalities will be reported to your doctor.
Physiotherapy
The Physiotherapist is the member of the rehabilitation team concerned with maximising your mobility and quality of life. On admission your Physiotherapist will assess your condition and, together with you, decide on achievable goals. A treatment program may include gait training, balance activities, exercises and endurance work. You may attend the physiotherapy gym six days a week as necessary. Generally, there are two physiotherapy sessions five days per week. Nursing staff will assist you (if required) to be showered, dressed and ready to participate in therapy sessions by 9am. Patients will also be given an exercise program that they are to initiate at other times during the day.
Alternatively, you may wish to see a private physiotherapist for 1:1 sessions. Your ward physiotherapist can help you source an appropriate private physiotherapist if needed. This will incur an out of pocket expense, with the cost dependent on your level of extras cover on your health insurance and the consultation fee of your specific physiotherapy clinic.
Depending on your private health care insurance cover you may also be eligible for physiotherapy in the home, where a physiotherapist from an external provider attends your house 1-2 times a week. Please talk with your ward physiotherapist early in your admission if you are interested in this option.
Occupational Therapy
An Occupational Therapist (OT) assists patients to achieve independence in their daily activities. Your OT will meet with you on admission and design an individual program to help you achieve your goals. Your OT may focus on the skilful use of your upper limbs and your thinking and memory. Your OT may suggest modified tasks or the use of equipment to assist you to do things for yourself. OT services may include relaxation classes, education in saving energy and making tasks easier and tips for preventing falls at home. You may need some modifications, installations or equipment in your home to make it safe. Your OT may offer a home visit to assess what is needed, help you to obtain the equipment and help arrange any modifications or installations.

Appendix 4 mobility aids and personal care
Showering
- Sit on a chair or stool if required. If you are not feeling tired or losing your balance whilst showering you are allowed to stand.
- Hold onto rails if available especially when closing your eyes.
- Place a non-slip mat inside the shower recess to reduce your falls risk.
- Do not attempt to get into a bath. Please discuss this with an occupational therapist if your only option is a shower over the bath.
Dressing
- Always get dressed sitting down on an appropriate height chair or bed.
- For lower limb dressing slip operated leg into pants first, followed by un-operated leg.
- For bilateral hips, use the easy reacher to pull the clothes over your feet and up to your knees.
- Stand up and pull the clothes up over your hips.
- If available, have someone help you with socks and TED stocking or use relevant equipment as advised by occupational therapists.
Chair
- Make sure your chair has a firm seat and back. It should also have arms for support and be at the correct height as advised by your therapist.
- A hi-lite armchair is often useful if you have no appropriate chairs at home and occupational therapists on the ward can advise you where you can hire these.
- Be mindful of the chairs you sit on when out in the community eg check that they are at the correct height and have arms.
Toilet
- For single and bilateral hip replacements an over the toilet aid or toilet surround may be required to increase your safety and independence when getting on and off the toilet.
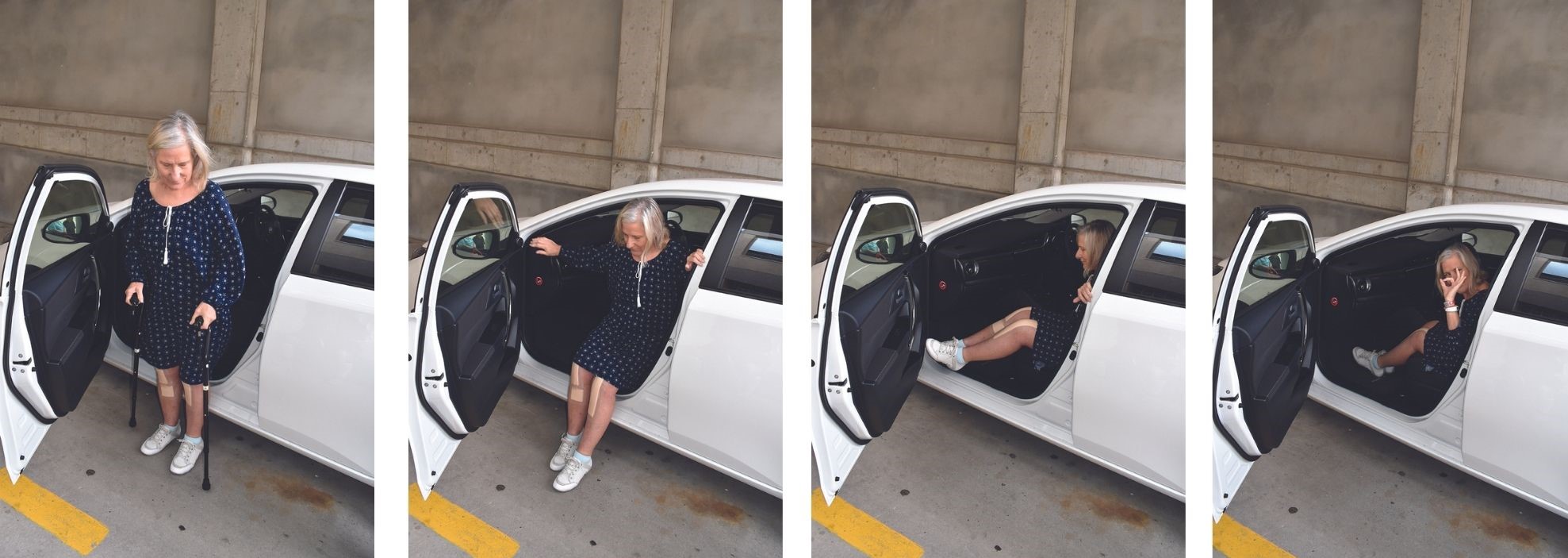
Appendix 5- Car Transfers- how to get in and out safely
- Have the driver position the car far enough away from the kerb so that you can get in and out on road level, with the door fully open.
- Ensure the passenger seat is pushed fully back and the back rest reclined to a 45 degree angle. If you have been advised to use a wedge cushion ensure it is on the seat.
- With the passenger door open, walk up to the car with your walking aid. When close to the car, turn so you have your back to the seat and can feel the seat/ door frame on the back of your legs (facing away from the car).
- Gently lower yourself down, keeping your operated leg extended. Hold on to the car uprights for support.
- Lean back and slide towards the middle of the car. Keep your body in a straight line as you pivot on your bottom to face the front of the car. Remember not to twist. Keep your legs close together as you bring them into the car. Bring the back rest up to a comfortable position when travelling.
- If you find it difficult to slide your legs into the car, you can lift your legs individually. Remember not to lean forwards or twist. You may want someone with you to assist with lifting your legs into the car for the first few times.
To transfer out of the car, use the above procedure in reverse.
Do not drive for the first six weeks following surgery or until you have been told to do so by your surgeon. Contact your insurance company to check when you are able to resume driving.
Car parking
St Vincent’s Private Hospital has several car parking areas for patients, visitors and staff. Paid parking is available in the Scott Street car park, which is located behind the Impressions on Scott café (opposite Entrance 2 in Scott Street) as well as in the Entrance 4 car park located at the rear of the hospital and accessed from Curzon Street. This car park has special designated areas for Day Surgery patients and a special drop off area for maternity patients.
Car parking tickets can be purchased through ticketing machines situated within the car parks and signs explain the parking zones and payment options.
Nominal fees apply for patients and visitors:
- 0-2 hours: $4
- 2-3 hours: $6
- 3+ hours: $8 (up to 12 hours)
- 24 hours: $15
Disabled parking is located near Entrances 1, 2, 3 and 4.
Parking in the streets surrounding the hospital is administered by the Toowoomba Regional Council and is free for up to three hours.
It normally takes three to four months for the swelling to settle down. Continue to put ice on your knee and have your knee elevated for 20 minute periods throughout the day by lying down, especially after exercising and long walks. Although the swelling does limit your knee bending, it is detrimental to your knee to wait until the swelling has gone away before you start pushing your knee to bend, as the scar tissue in your knee will have developed by that time, causing a permanent restriction in knee bending. You may begin cycling on a stationary bike two weeks after your operation. After six weeks you may begin using weights on your legs. You should begin with low weights and gradually increase them. Check with your physiotherapist prior to beginning weights or gym work. It is not advisable to do any regular jogging, running or jumping activities after your surgery as it will cause your knee replacement to wear more quic
Related Content

Patient Information & Safety- Admission Information
Information about patient admission at St Vincent's Private Hospital Toowoomba.
Read More
Orthopaedics- Hip Replacement
Information for patients having hip replacement surgery at St Vincent's Toowoomba.
Read More
Rehabilitation Services
Information about rehabilitation services at St Vincent's Toowoomba.
Read More