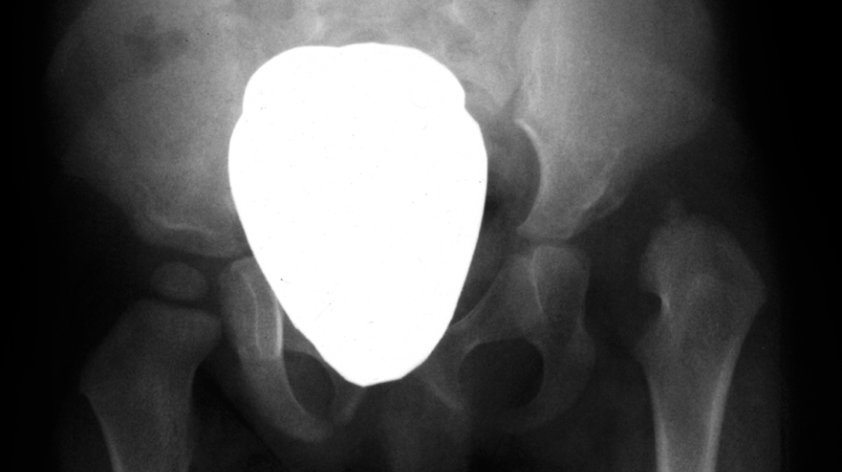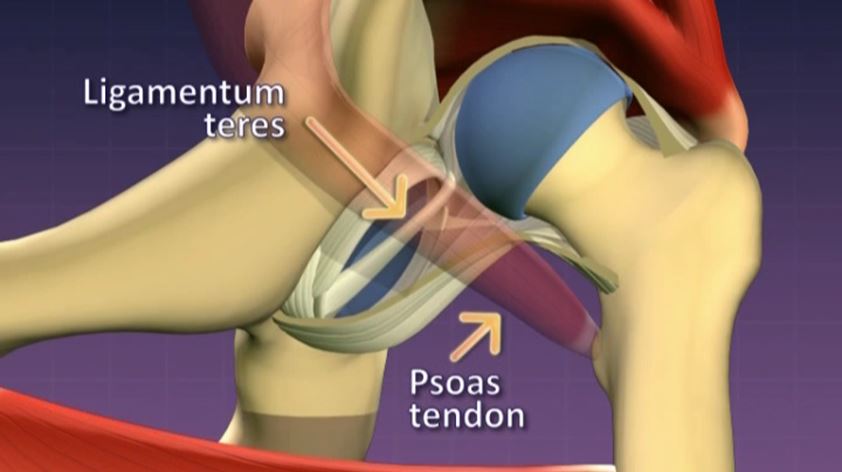
Anatomy of a dislocated hip

Risk factors
- Female sex account for nearly 80% of cases of DDH - it is thought that the affect of maternal hormones on the foetus predisposes females to ligamentous laxity.
- Family History of DDH - although not following a recognised genetic inheritance pattern, the incidence of DDH increases if a first degree relative has been affected
- Breech presentation - results in extreme flexion and limitation of hip motion causing capsular stretching and acetabular dysplasia.
- Intrauterine packaging problems - a relative reduction in uterine volume may result in a number of so called “packaging disorders” during which DDH may occur. e.g plagiocephaly, congenital muscular torticollis, foot deformities (metatarsus adductus, calcaneovalgus)
- Wrapping or swaddling - there is clear evidence that the practice of comfort wrapping that included the infants legs is extremely detrimental to the hips development and directly associated with the development of dysplasia and dislocation
However, it should be noted that more than 60% of infants with DDH have no identifiable risk factors.

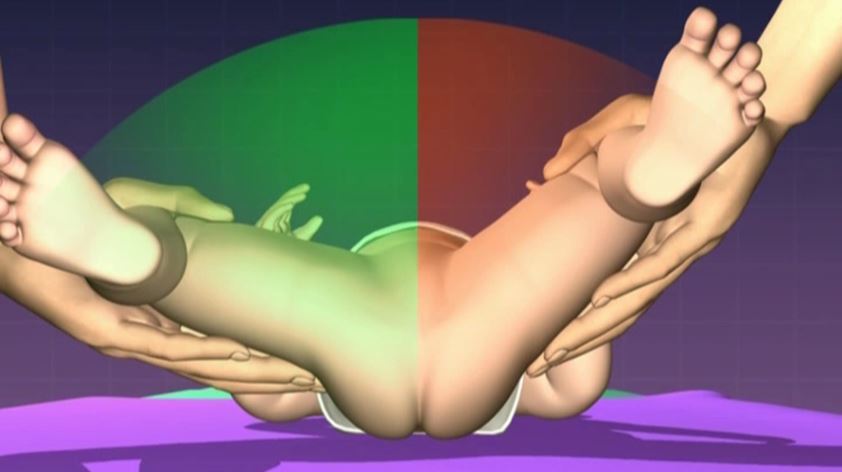
Barlow Test

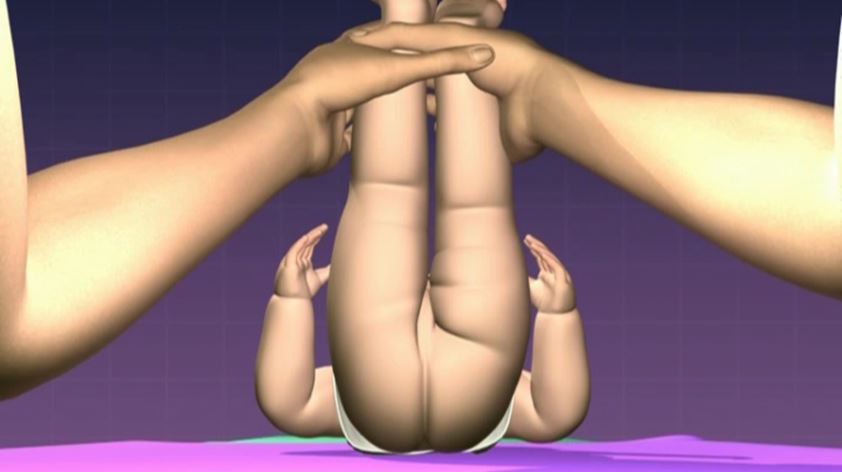
Ortolani Test
Gluteal Fold Asymmetry